Four Jobs I have Had
* jewelry counter at a department store
* nanny
* residential counselor
* nursing assistant
Four Places I Have Lived:
* my hometown
* the town I live in now, the best town in the world!
* Seattle, WA
* bumming around
Four Movies I Could Watch Again and Again:
* The Princess Diaries
* Center Stage
* Point Break
* Blue Crush
Four Television Shows I Love:
* Bones
* 2 Broke Girls
* Parks and Recreation
* Top Chef
Four Authors I Enjoy:
* Mary Roach
* Poppy Z. Brite
* Jen Lancaster
* Meg Cabot
Four Places I Have Travelled To:
* San Diego, CA
* Whistler, BC
* Bend, OR
* Austin, TX
Four Website I Visit Daily:
* http://tumblr.com
* http://www.allnurses.com
* http://www.facebook.com
* http://www.pandora.com
Four Blogs I Visit Weekly:
* Cake Wrecks www.cakewrecks.com/
* The Bloggess www.thebloggess.com
* Clinical Psychology and Psychiatry http://clinpsyc.blogspot.com/
* Head Nurse http://head-nurse.blogspot.com/
Four of My Favorite Foods:
* Rice
* smoothies with fruit and vanilla soymilk
* peanut butter
* miso soup
Four Places I'd Rather Be:
* at a beach
* Los Angeles
* camping with Mr. Polly
* in nursing school for my BSN
Four People I Want to Tag:
* Zazzy http://frazzledrazzlern.blogspot.com/
* Estelle Darling www.estelledarling.blogspot.com/
* Annie http://arkansasisyourkansas.blogspot.com/
* Jess http://icosmeticrn.blogspot.com/
Wednesday, February 29, 2012
Tuesday, February 28, 2012
Fall Risks and restraints
The culture of nursing homes and assisted living facilities has shifted far away from the use of restraints; most places are restraint-free by law these days. The hospital is one of the only places I can imagine restraints remaining in use, and that is simply because of the acuity (how sick) our patients there are. They cannot afford to be pulling out the lines that are giving them IV antibiotics and blood transfusions, because without those things, they will die.
Even at the hospital, restraints are considered a last resort. They frequently utilize one-to-one 'sitters' to watch and maintain safety of very difficult patients. I was pulled from my regular duties to act as one last night, for a confused elderly person who would not stop climbing out of bed (and was a fall risk), pulling out lines, and removing their much-needed supplementary oxygen tubing. Even with me there, the patient was very agitated, and trying to literally climb over the furniture to get out of the bed. I was willing to let her get up, but she was so damn fast she was apt to get away before I could gather up all the things that were attached to her so I could ferry them along after her to prevent them from ripping out.
Finally the MD returned the page from the nurse, and ordered a small dose of an antipsychotic. It didn't stop the patient from trying to get up, it just calmed the patient down enough to stop physically shoving me out of the way, which was good enough.
This was one of those situations where I think that chemical restraints would be so much more effective than physical. My patient has such poor short-term memory that s/he would forget what I had said literally 20 seconds before. Putting someone like that in physical restraints is going to be a huge safety risk because they're still anxious and panicky and energetic, and will focus all of that onto getting out of the restraints one way or another.
Whereas a strong sedative seems highly appropriate and could allow this person the time to absorb their antibiotics, fluids, and oxygen in order to begin healing.
Unfortunately, I don't think we have a specific policy and protocol for chemical restraints the way we do for physical ones. I understand they're risky in terms of oversedation; you don't want to accidentally kill someone! But I wonder, if I were the physician getting paged in the middle of the night, whether I'd view the sedatives I'm prescribing as restraints or 'sleep aids' or what?
Even at the hospital, restraints are considered a last resort. They frequently utilize one-to-one 'sitters' to watch and maintain safety of very difficult patients. I was pulled from my regular duties to act as one last night, for a confused elderly person who would not stop climbing out of bed (and was a fall risk), pulling out lines, and removing their much-needed supplementary oxygen tubing. Even with me there, the patient was very agitated, and trying to literally climb over the furniture to get out of the bed. I was willing to let her get up, but she was so damn fast she was apt to get away before I could gather up all the things that were attached to her so I could ferry them along after her to prevent them from ripping out.
Finally the MD returned the page from the nurse, and ordered a small dose of an antipsychotic. It didn't stop the patient from trying to get up, it just calmed the patient down enough to stop physically shoving me out of the way, which was good enough.
This was one of those situations where I think that chemical restraints would be so much more effective than physical. My patient has such poor short-term memory that s/he would forget what I had said literally 20 seconds before. Putting someone like that in physical restraints is going to be a huge safety risk because they're still anxious and panicky and energetic, and will focus all of that onto getting out of the restraints one way or another.
Whereas a strong sedative seems highly appropriate and could allow this person the time to absorb their antibiotics, fluids, and oxygen in order to begin healing.
Unfortunately, I don't think we have a specific policy and protocol for chemical restraints the way we do for physical ones. I understand they're risky in terms of oversedation; you don't want to accidentally kill someone! But I wonder, if I were the physician getting paged in the middle of the night, whether I'd view the sedatives I'm prescribing as restraints or 'sleep aids' or what?
Wednesday, February 22, 2012
Suicide watch
The other night at the hospital, I got sent to a different floor than my usual one to do a one-on-one suicide watch for a patient waiting for a transfer to our psych unit.
My patient was very pleasant, and very very sad, and rather nuts.
And that experience clinched it for me - no psych nursing for me, thanks. Geropsych, possibly (I just love old people enough to overcome my aversion to the wild behavior). But regular psych, where someone is sharing their terrible childhood and depression and I just want to cry and cry for them? No thanks.
On the plus side, I learned to play Yahtzee and it's so fun!
Also, I like that we live in a world where someone very poor with no family to speak of will get round-the-clock care to keep that individual alive and stable with a goal of recovery ahead of them. And there's no profit in doing so. We just do it because it's the right thing to do.
That's a good thought to hold on to.
My patient was very pleasant, and very very sad, and rather nuts.
And that experience clinched it for me - no psych nursing for me, thanks. Geropsych, possibly (I just love old people enough to overcome my aversion to the wild behavior). But regular psych, where someone is sharing their terrible childhood and depression and I just want to cry and cry for them? No thanks.
On the plus side, I learned to play Yahtzee and it's so fun!
Also, I like that we live in a world where someone very poor with no family to speak of will get round-the-clock care to keep that individual alive and stable with a goal of recovery ahead of them. And there's no profit in doing so. We just do it because it's the right thing to do.
That's a good thought to hold on to.
Thursday, February 16, 2012
Studying: it works!
I think I mentioned recently that after finding out that my employment at Father Sainty's is no longer such a gigantic helping factor in getting me into nursing school, I decided I needed to pull my grades up. I was getting a B in Anatomy and Physiology and an A- in Bio. That B in A&P was sort of tenouous, though, since I'd gotten a B- on my most recent exam.
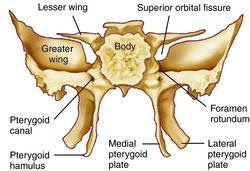
I studied like crazy for my most recent exam on bones, and got a 90% on it! If I continue to study this hard and do that well on my remaining exams this quarter, I should be able to get my grade up to an A-, I think. So that's my plan.
Too bad I don't love muscles the way I love bones. I even had dreams regarding specific bones (I was in a butterfly garden but the butterflies were sphenoid bones that were flying around, and I was delighted!).
So while it may be tempting to put work first, I need to remember to put school first. That means if I have to sleep less to study more, that's what will happen. If it means showing up at work exhausted rather than after napping, then that's the deal. If it means eating dinner in the cafeteria instead of cooking and packing my meals, that's okay too.
After this quarter I only have to do A&P II and microbiology. I think I can technically apply to nursing school even with one class left to finish up, so maybe I can apply for admittance next Winter quarter and take microbiology in the fall before it begins?
Either way, I plan to stop working at the GreatRep once I'm in nursing school. That 10-hour workday is just too much time lost. If I can take out loans, i'll do that to compensate for the lost income. I know how incredibly lucky I am to be going to school for free right now, and I know that won't continue forever.
More and more the idea of goign for my LPN and working in a skilled nursing facility or inpatient rehab sounds appealing to me. If I'm going to work and go to school, part of me thinks that work should be the best-paying I'm able to get.
Either way, I'm back on board with school!
And here's a visual for anyone wondering about my dreams: they're a cross between this

and this
I studied like crazy for my most recent exam on bones, and got a 90% on it! If I continue to study this hard and do that well on my remaining exams this quarter, I should be able to get my grade up to an A-, I think. So that's my plan.
Too bad I don't love muscles the way I love bones. I even had dreams regarding specific bones (I was in a butterfly garden but the butterflies were sphenoid bones that were flying around, and I was delighted!).
So while it may be tempting to put work first, I need to remember to put school first. That means if I have to sleep less to study more, that's what will happen. If it means showing up at work exhausted rather than after napping, then that's the deal. If it means eating dinner in the cafeteria instead of cooking and packing my meals, that's okay too.
After this quarter I only have to do A&P II and microbiology. I think I can technically apply to nursing school even with one class left to finish up, so maybe I can apply for admittance next Winter quarter and take microbiology in the fall before it begins?
Either way, I plan to stop working at the GreatRep once I'm in nursing school. That 10-hour workday is just too much time lost. If I can take out loans, i'll do that to compensate for the lost income. I know how incredibly lucky I am to be going to school for free right now, and I know that won't continue forever.
More and more the idea of goign for my LPN and working in a skilled nursing facility or inpatient rehab sounds appealing to me. If I'm going to work and go to school, part of me thinks that work should be the best-paying I'm able to get.
Either way, I'm back on board with school!
And here's a visual for anyone wondering about my dreams: they're a cross between this

and this

Wednesday, February 15, 2012
Best of Both?
I had a rough, rough shift at work last night. Was working with a nurse that is new to our floor, and coming from a floor that's notorious for having RN/CNA conflicts up the wazzoo. So I made time to sit and catch up with NewNurse when he came on shift halfway through mine. I already had 13-14 patients of my own, and the way we have it set up, all the call lights come to the CNA's first. If we don't answer, then they are forwarded on to that patient's nurse. So you can imagine how busy I am on these nights. Of my 13-14 patients, I'm likely to have at least 5 diabetics who need their blood sugar checked before meals and at bedtime. Another 2-3 who are confused/fall risk/non-English speaking. And 4 or 5 who are fresh post-ops, which means they're in a lot of pain, bed bound, and possibly needing to be strapped in and out of devices to move or steady their joints.
NewNurse got pissed at me for two things, one of which I think was valid (although I had no way of knowing about it) and the other which was absolutely not; one of our regular floor nurses scoffed at NewNurse when she heard him getting angry at me about it in the nurses' station.
Anyway, everything turned out fine, all my patients were okay (although one did give me a terrible scare, then when it became clear that my fear had been because of one of the machines giving a wrong reading the first time, the patient asked "Are we in trouble? I'll cover for us. What should I say?" which made me laugh despite how upset I'd been).
But I'm now mentally comparing that to my shift last week when I filled in over at the inpatient rehab unit (physical rehabilitation, not drug or alcohol rehab). I had such a mellow night, I was able to cover most of the unit by myself. And if I got tied up with something, the nurses were aware of it and went and did things for their patients themselves. I even had time to help a very sweet older lady get her Kindle working again, which delighted her!
It was more like a nursing home, in that it's lower acuity and the patients are there for longer periods of time. But it's a smaller unit, so that makes teamwork easier. And it pays at the rate of the hospital, not at the rate of a nursing home.
Is inpatient rehab the best of both worlds? Less stress, more time with patients, and the same pay and benefits?
Could be...
NewNurse got pissed at me for two things, one of which I think was valid (although I had no way of knowing about it) and the other which was absolutely not; one of our regular floor nurses scoffed at NewNurse when she heard him getting angry at me about it in the nurses' station.
Anyway, everything turned out fine, all my patients were okay (although one did give me a terrible scare, then when it became clear that my fear had been because of one of the machines giving a wrong reading the first time, the patient asked "Are we in trouble? I'll cover for us. What should I say?" which made me laugh despite how upset I'd been).
But I'm now mentally comparing that to my shift last week when I filled in over at the inpatient rehab unit (physical rehabilitation, not drug or alcohol rehab). I had such a mellow night, I was able to cover most of the unit by myself. And if I got tied up with something, the nurses were aware of it and went and did things for their patients themselves. I even had time to help a very sweet older lady get her Kindle working again, which delighted her!
It was more like a nursing home, in that it's lower acuity and the patients are there for longer periods of time. But it's a smaller unit, so that makes teamwork easier. And it pays at the rate of the hospital, not at the rate of a nursing home.
Is inpatient rehab the best of both worlds? Less stress, more time with patients, and the same pay and benefits?
Could be...
Sunday, February 12, 2012
A piano fell on my head.
I am so frustrated right now. One of the main reasons I applied at the hospital (apart from benefits and pay) is that the hospital has a relationship with the community college (where I intended to go get my RN) where a certain percentage of the seats in the RN program are reserved for hospital employees, and where in turn, the hospital will help pay your tuition at school provided you agree to work for them for one year to help 'repay' that tuition.
I just got an email that the hospital is ending that relationship, becuase they no longer have a shortage of RN's in the area. Friiiiiiiiiick.
I think the educational assistance may still be in effect but is probably harder to get. And this means that I am now competing with the general public for admission to any nursing school. So I better be hitting the books for my prereqs.
I know, not the end of the world. But not news that I'm happy about at all. Not at all.
I just got an email that the hospital is ending that relationship, becuase they no longer have a shortage of RN's in the area. Friiiiiiiiiick.
I think the educational assistance may still be in effect but is probably harder to get. And this means that I am now competing with the general public for admission to any nursing school. So I better be hitting the books for my prereqs.
I know, not the end of the world. But not news that I'm happy about at all. Not at all.
Wednesday, February 1, 2012
Mountain, not a molehill
Today I'm feeling like I've bitten off more than I can chew this quarter. I'm taking Anatomy and Physiology I, and an online bio course, so that's 10 credits total. I'm working full-time, 3 shifts a week at the hospital, and one at the Dementia Facility.
On a typical day, I get up at around 7:30, get ready, catch the bus to school, get home from school at around 11, and then study/eat/nap until time for work at 15:30-23:30. I try to get to sleep by 1am, then do it again the next day. And lord, am I tired. I've fallen asleep on the bus, nearly fell asleep in the bathroom at work last night (the auto flushing toilet woke me up with a start and I LEAPT to my feet!) and in general am just so tired and feel so behind on everything.
Next quarter, I'm going to only take one class because I can't afford to cut back on work and I want to really learn this stuff and do well in my classes.
There's all this weird drama in the nursing program at my Community College, where the previous director of the program just finally "stepped down" aka got fired, and a new one is taking her place. The new one is my academic advisor, and I like her quite a bit from what I know of her in that context, so hopefully she can turn this ship around. Right now the nursing program's retention rates and NCLEX pass rates are very poor. So in many ways I might be better off going to a different community college, but Father Sainty's will either help pay my tuition at my current community college or at the University. If I want to go to the University, there's a couple of extra prereqs I need to take (including Chem 131 - yikes) and it would be a long commute to take classes there all throughout nursing school.
Anyway, all of that is something I shouldn't be worrying about this early on. If I don't focus on the present my grades will suck so badly I won't be able to get into school.
Work is going pretty great though. I just (belatedly) had my 90-day evaluation at the hospital with my nurse manager, and it went quite well. I got some nice comments on my peer reviews including "Pollyanna is soft spoken and calming to patients" and one about how I'm pursuing my education and always happy to share new things I've learned. So those both make me feel really good!
I feel so, so lucky every day to be working on the floor I'm working on. Our charge nurses are awesome, the floor nurses are easy to work with and appreciative, and the majority of our patients are motivated to work hard toward their recovery goals and get back to their lives as soon as possible. I like being able to help them with that.
And this week in A&P we're going to start studying the skeletal system, which I'm very very happy about since I hear the terminology at work all the time (about fractures and where they are and what type and so on) but don't understand it. So I cannot WAIT to put cell respiration behind me and move on to something that feels more relevant to real life!
On a typical day, I get up at around 7:30, get ready, catch the bus to school, get home from school at around 11, and then study/eat/nap until time for work at 15:30-23:30. I try to get to sleep by 1am, then do it again the next day. And lord, am I tired. I've fallen asleep on the bus, nearly fell asleep in the bathroom at work last night (the auto flushing toilet woke me up with a start and I LEAPT to my feet!) and in general am just so tired and feel so behind on everything.
Next quarter, I'm going to only take one class because I can't afford to cut back on work and I want to really learn this stuff and do well in my classes.
There's all this weird drama in the nursing program at my Community College, where the previous director of the program just finally "stepped down" aka got fired, and a new one is taking her place. The new one is my academic advisor, and I like her quite a bit from what I know of her in that context, so hopefully she can turn this ship around. Right now the nursing program's retention rates and NCLEX pass rates are very poor. So in many ways I might be better off going to a different community college, but Father Sainty's will either help pay my tuition at my current community college or at the University. If I want to go to the University, there's a couple of extra prereqs I need to take (including Chem 131 - yikes) and it would be a long commute to take classes there all throughout nursing school.
Anyway, all of that is something I shouldn't be worrying about this early on. If I don't focus on the present my grades will suck so badly I won't be able to get into school.
Work is going pretty great though. I just (belatedly) had my 90-day evaluation at the hospital with my nurse manager, and it went quite well. I got some nice comments on my peer reviews including "Pollyanna is soft spoken and calming to patients" and one about how I'm pursuing my education and always happy to share new things I've learned. So those both make me feel really good!
I feel so, so lucky every day to be working on the floor I'm working on. Our charge nurses are awesome, the floor nurses are easy to work with and appreciative, and the majority of our patients are motivated to work hard toward their recovery goals and get back to their lives as soon as possible. I like being able to help them with that.
And this week in A&P we're going to start studying the skeletal system, which I'm very very happy about since I hear the terminology at work all the time (about fractures and where they are and what type and so on) but don't understand it. So I cannot WAIT to put cell respiration behind me and move on to something that feels more relevant to real life!
Subscribe to:
Posts (Atom)